Refusal Form - In this circumstance, consider asking the patient to sign. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. ____________________ from any and all liability. A record of the patient’s refusal of the treatment/testing plan or advice. “i am refusing to have these radiographs taken at this time.
____________________ from any and all liability. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. A record of the patient’s refusal of the treatment/testing plan or advice. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. “i am refusing to have these radiographs taken at this time. In this circumstance, consider asking the patient to sign.
By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. In this circumstance, consider asking the patient to sign. “i am refusing to have these radiographs taken at this time. A record of the patient’s refusal of the treatment/testing plan or advice. ____________________ from any and all liability. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme.

Informed Refusal Form Edit & Share airSlate SignNow
A record of the patient’s refusal of the treatment/testing plan or advice. In this circumstance, consider asking the patient to sign. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. ____________________ from any and all liability. _____________________________________________ i am provided with this refusal form and information so i may understand.
Waiver Of Right Of First Refusal Template
_____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. A record of the patient’s refusal of the treatment/testing plan or advice. In this circumstance, consider asking the patient to sign. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by..

Medical Treatment Refusal Form Template amulette
This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. ____________________ from.

Refusal of treatment form pdf Fill out & sign online DocHub
____________________ from any and all liability. “i am refusing to have these radiographs taken at this time. A record of the patient’s refusal of the treatment/testing plan or advice. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. In this circumstance, consider asking the patient to sign.
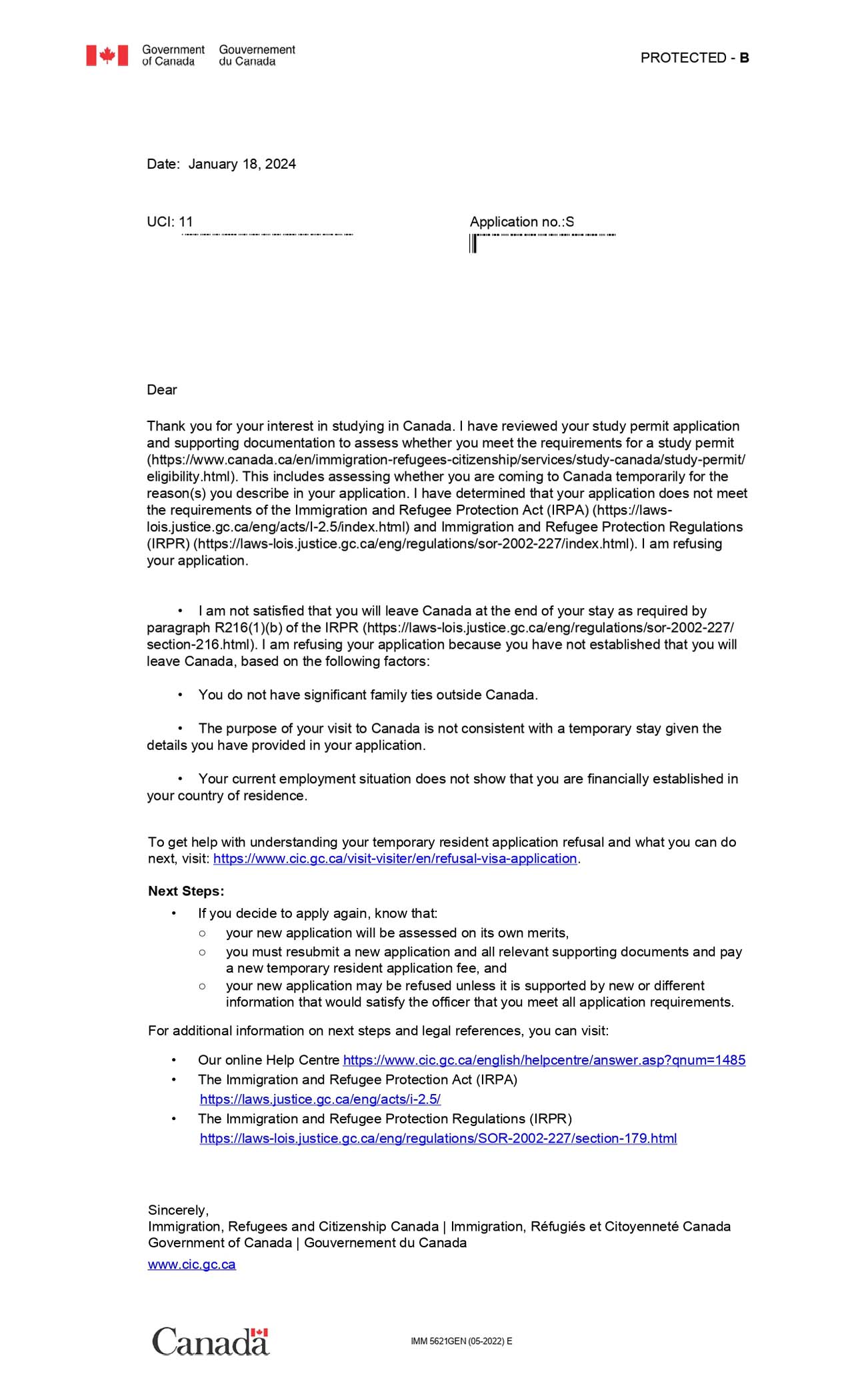
Canada Visa Refusal Immigration Refusal Lawyers
A record of the patient’s refusal of the treatment/testing plan or advice. ____________________ from any and all liability. _____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. “i am refusing to have these.

Medical Treatment Refusal Form Template amulette
By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. A record of the patient’s refusal of the treatment/testing plan or advice. In this circumstance, consider asking the patient to sign. ____________________ from any and all liability. “i am refusing to have these radiographs taken at this time.

Vaccine Refusal Form Template Jotform
_____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. “i am refusing to have these radiographs taken at this time. By signing below, i understand that my refusal to follow.
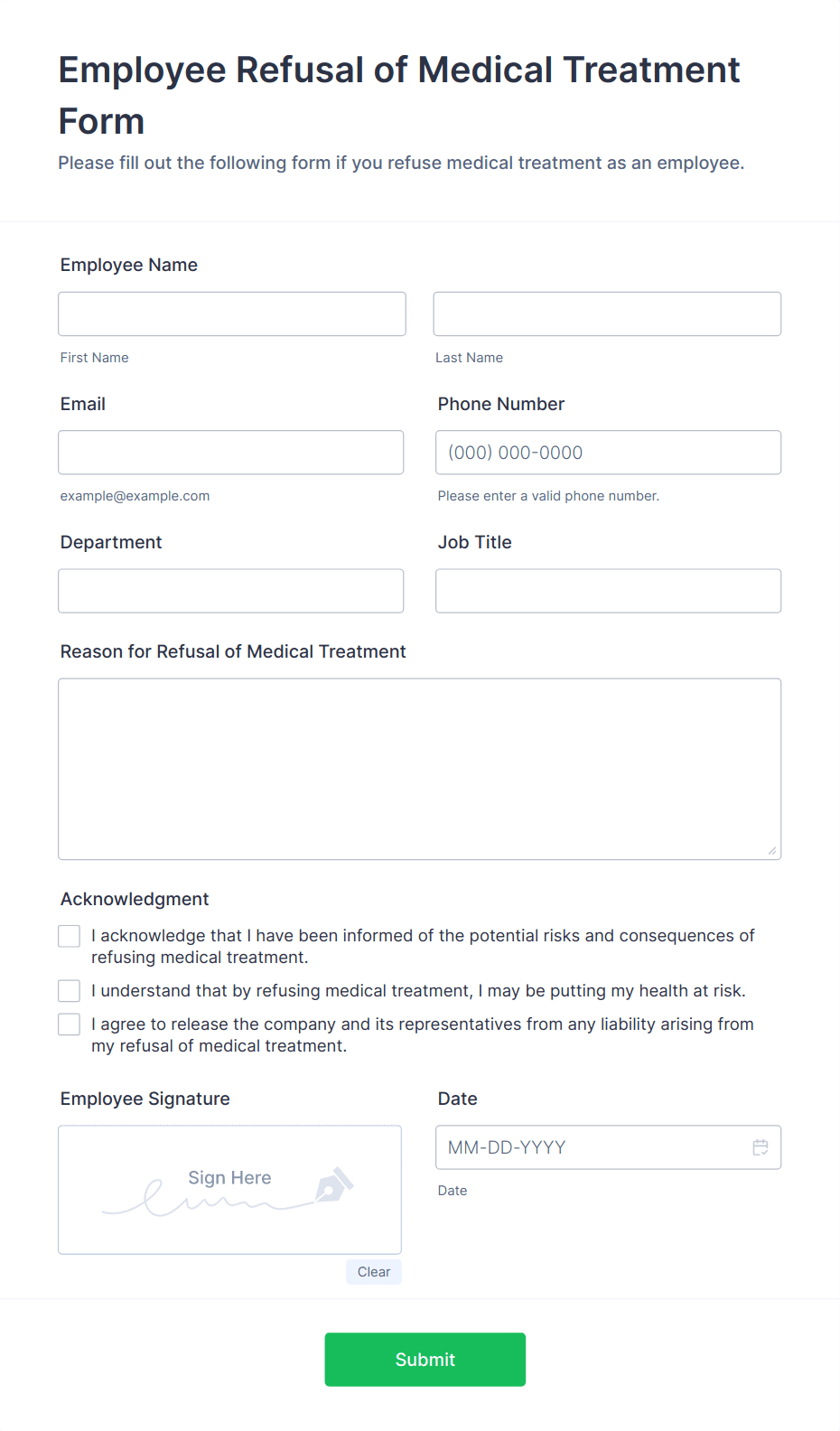
Employee Refusal of Medical Treatment Form Template Jotform
In this circumstance, consider asking the patient to sign. A record of the patient’s refusal of the treatment/testing plan or advice. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. ____________________ from any and all liability. _____________________________________________ i am provided with this refusal form and information so i may understand.
First Refusal Complete with ease airSlate SignNow
“i am refusing to have these radiographs taken at this time. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could. In this circumstance, consider asking the patient to sign. A record of the patient’s refusal of the treatment/testing plan or advice. ____________________ from any and all liability.
Refusal of Medical Treatment Media Services Fill Out and Sign
____________________ from any and all liability. “i am refusing to have these radiographs taken at this time. A record of the patient’s refusal of the treatment/testing plan or advice. In this circumstance, consider asking the patient to sign. By signing below, i understand that my refusal to follow my providers advice and undergo the recommended test/treatment/procedure could.
A Record Of The Patient’s Refusal Of The Treatment/Testing Plan Or Advice.
“i am refusing to have these radiographs taken at this time. This form should be signed by the patient or authorized party if he/she refuses any surgical procedure or medical treatment recommended by. ____________________ from any and all liability. In this circumstance, consider asking the patient to sign.
By Signing Below, I Understand That My Refusal To Follow My Providers Advice And Undergo The Recommended Test/Treatment/Procedure Could.
_____________________________________________ i am provided with this refusal form and information so i may understand the recommended treatme.