Psychotropic Medication Consent Form - ☐ client gives verbal consent, but unwilling or unable to sign. I understand that once the targeted symptom or behavior is controlled, the usage of. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. ☐ client gives consent to this treatment plan for psychotropic medications. I give my full consent for the use of the medication indicated above. Hereby give my consent to treatment with this medication. I agree to notify my practitioner with any changes or problems with my medications. I understand that i may seek additional information, and that i may.
By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. I understand that i may seek additional information, and that i may. ☐ client gives consent to this treatment plan for psychotropic medications. I understand that once the targeted symptom or behavior is controlled, the usage of. I agree to notify my practitioner with any changes or problems with my medications. ☐ client gives verbal consent, but unwilling or unable to sign. Hereby give my consent to treatment with this medication. I give my full consent for the use of the medication indicated above.
I give my full consent for the use of the medication indicated above. I understand that i may seek additional information, and that i may. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. ☐ client gives consent to this treatment plan for psychotropic medications. ☐ client gives verbal consent, but unwilling or unable to sign. Hereby give my consent to treatment with this medication. I understand that once the targeted symptom or behavior is controlled, the usage of. I agree to notify my practitioner with any changes or problems with my medications.
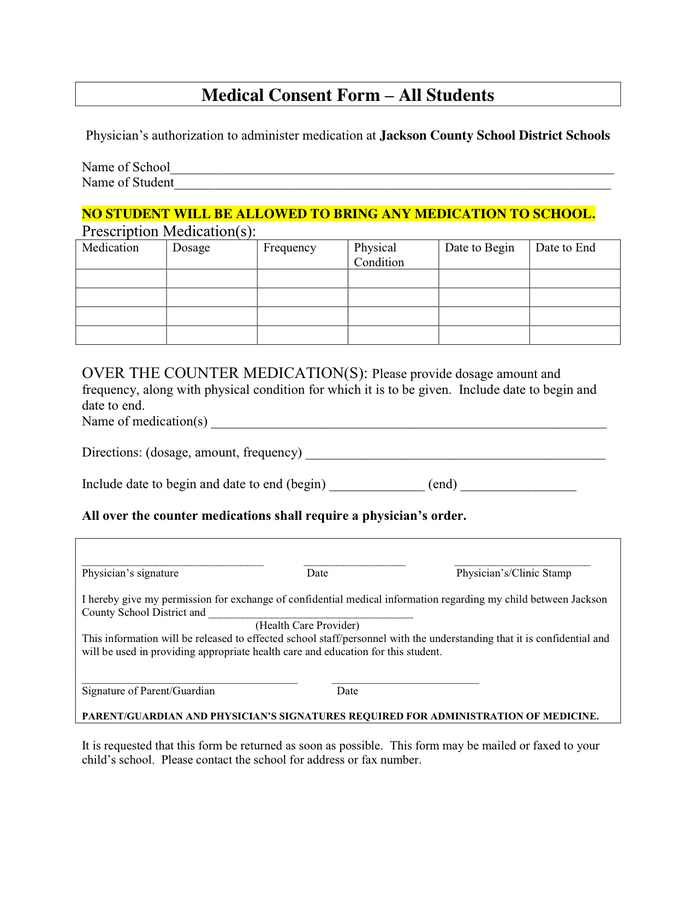
Medical Consent Form download free documents for PDF, Word and Excel
Hereby give my consent to treatment with this medication. ☐ client gives verbal consent, but unwilling or unable to sign. ☐ client gives consent to this treatment plan for psychotropic medications. I understand that once the targeted symptom or behavior is controlled, the usage of. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section.
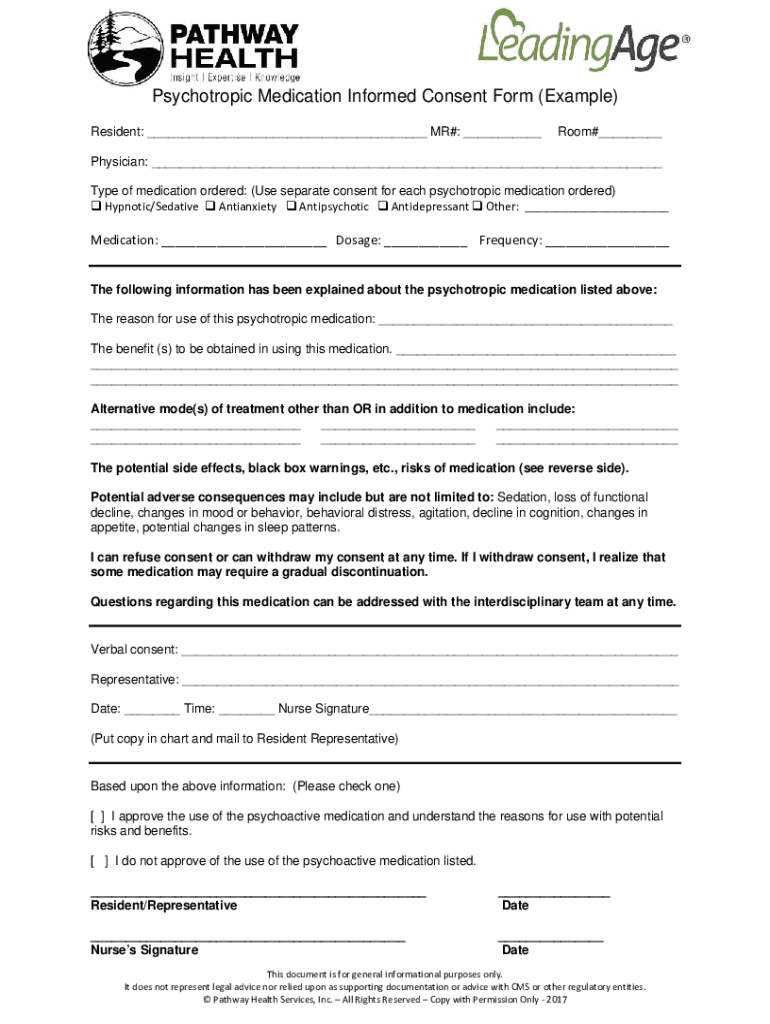
Fillable Online Sample Psychotropic Medication Informed Consent Form
I agree to notify my practitioner with any changes or problems with my medications. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. I understand that once the targeted symptom or behavior is controlled, the usage of. I give my full consent for the use of the medication indicated above. ☐ client.
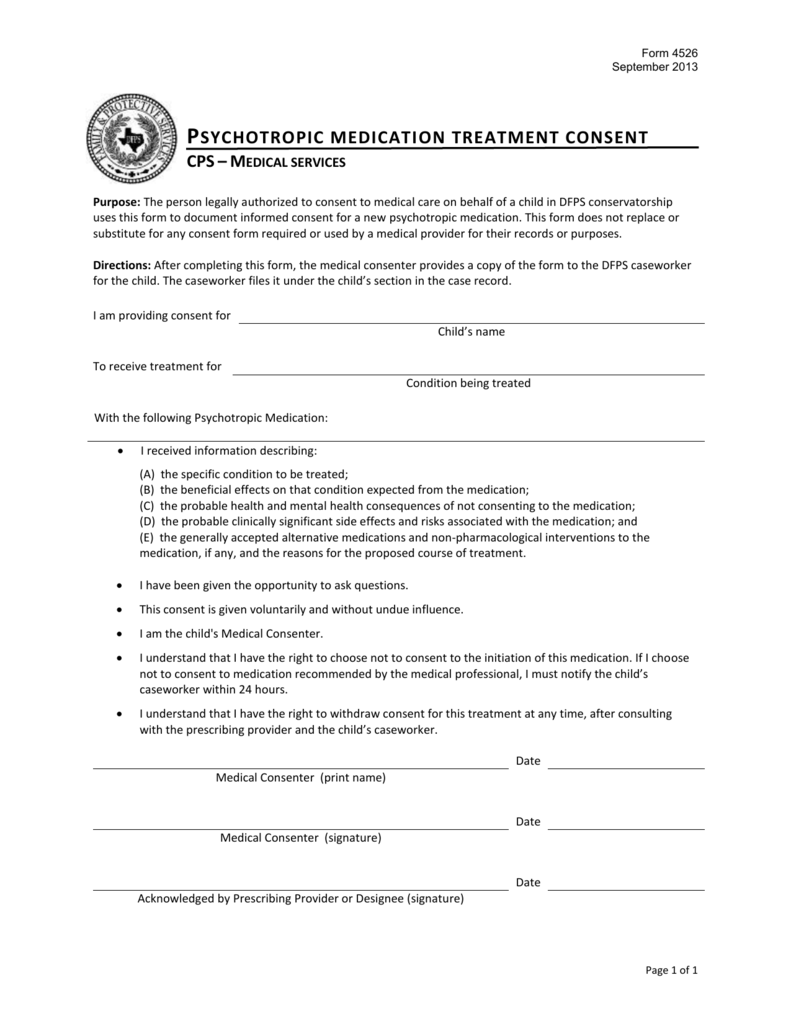
Psychotropic Medication Treatment Consent Form(4526)
Hereby give my consent to treatment with this medication. ☐ client gives verbal consent, but unwilling or unable to sign. I agree to notify my practitioner with any changes or problems with my medications. I understand that once the targeted symptom or behavior is controlled, the usage of. I give my full consent for the use of the medication indicated.
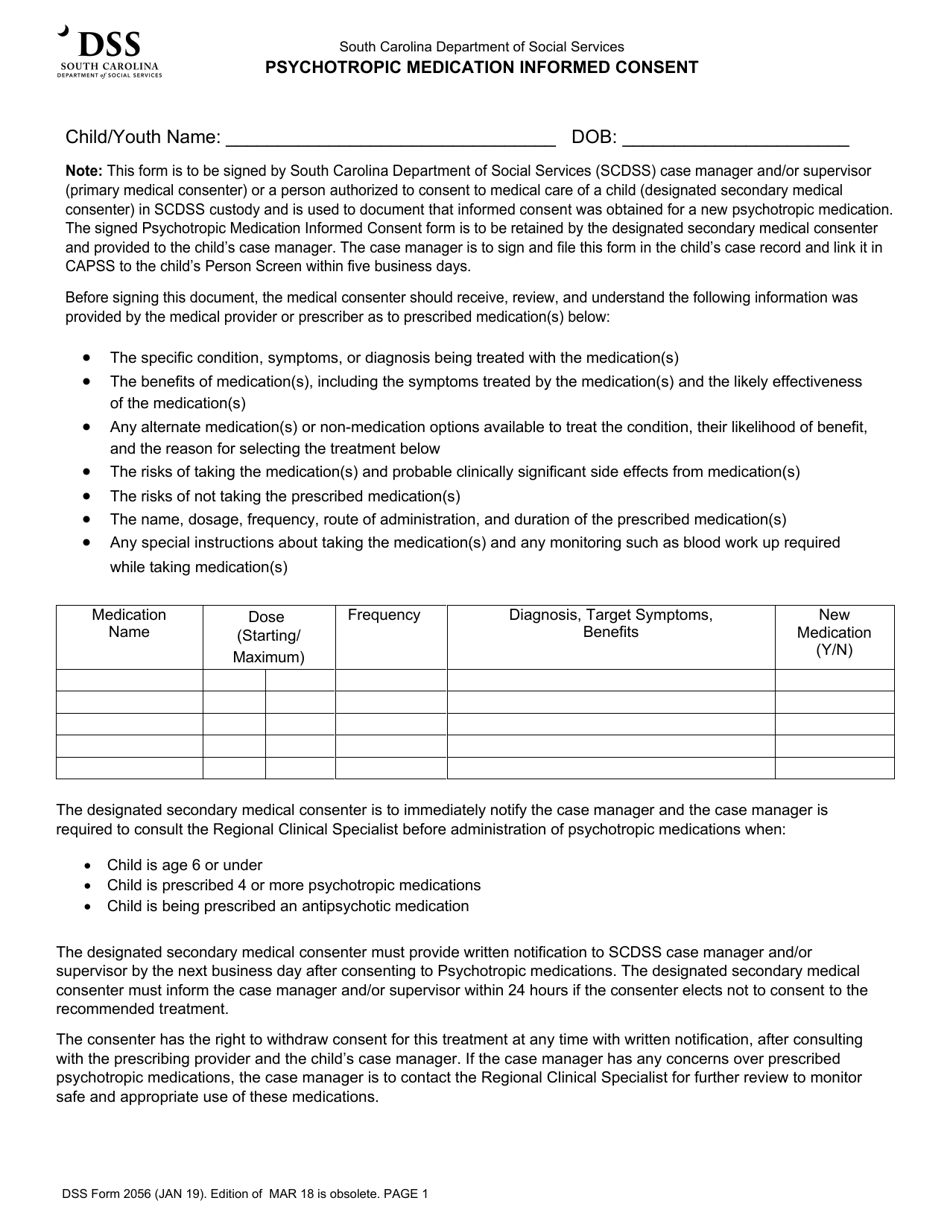
DSS Form 2056 Fill Out, Sign Online and Download Fillable PDF, South
Hereby give my consent to treatment with this medication. I understand that i may seek additional information, and that i may. ☐ client gives verbal consent, but unwilling or unable to sign. I understand that once the targeted symptom or behavior is controlled, the usage of. I agree to notify my practitioner with any changes or problems with my medications.

Medication consent Fill out & sign online DocHub
I understand that once the targeted symptom or behavior is controlled, the usage of. I give my full consent for the use of the medication indicated above. I understand that i may seek additional information, and that i may. ☐ client gives consent to this treatment plan for psychotropic medications. ☐ client gives verbal consent, but unwilling or unable to.

Psychotropic Medication Consent CF 0173 C 1/15 Doc Template pdfFiller
I give my full consent for the use of the medication indicated above. I understand that once the targeted symptom or behavior is controlled, the usage of. ☐ client gives verbal consent, but unwilling or unable to sign. ☐ client gives consent to this treatment plan for psychotropic medications. By signing below, i give consent for __________________________________________________________ to receive the.
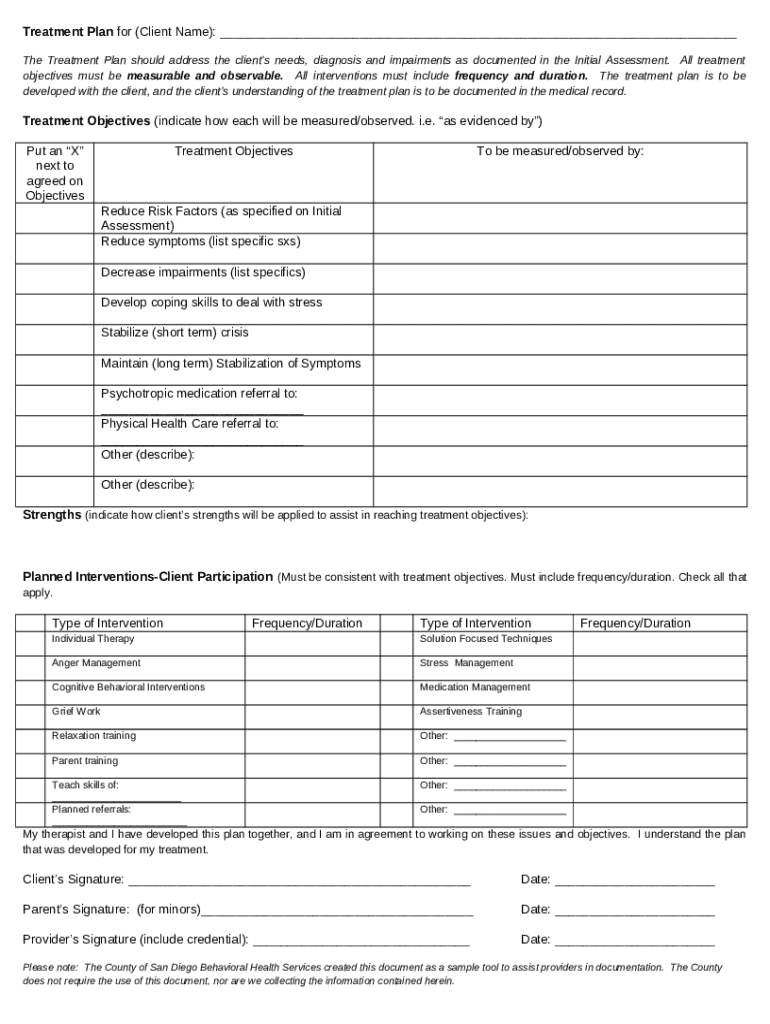
Treatment Plan and Ined Consent for Psychotropic Medical Doc Template
I give my full consent for the use of the medication indicated above. Hereby give my consent to treatment with this medication. I understand that i may seek additional information, and that i may. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. ☐ client gives verbal consent, but unwilling or unable.
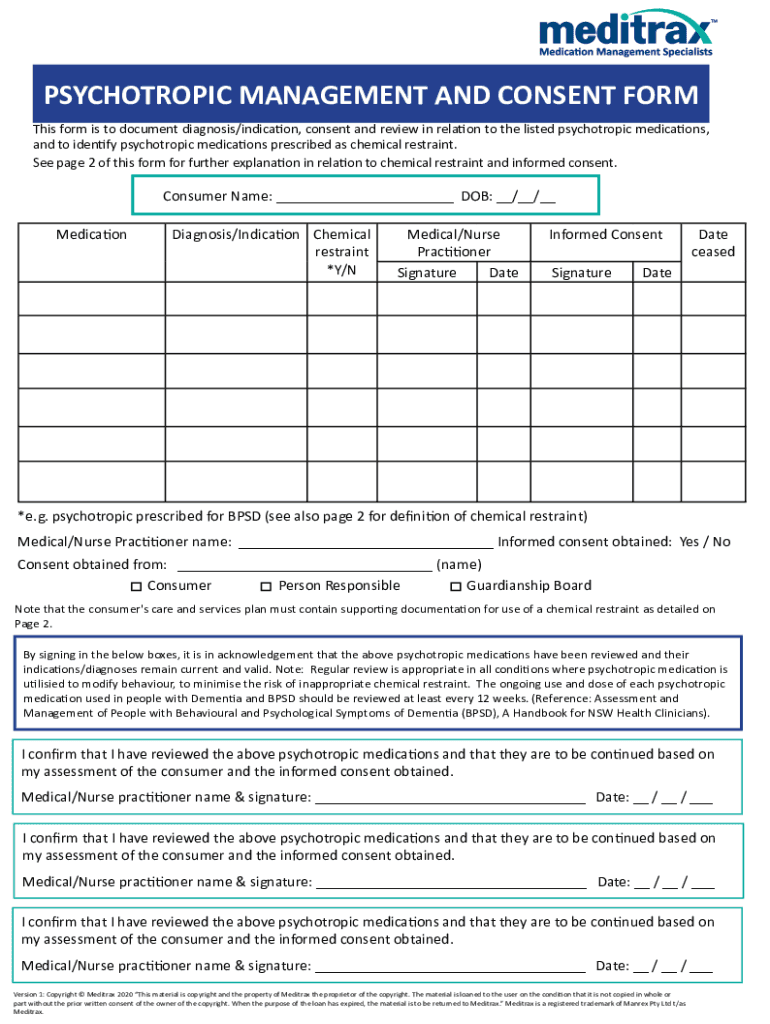
Fillable Online PSYCHOTROPIC MANAGEMENT AND CONSENT FORM Fax Email
By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. I understand that i may seek additional information, and that i may. ☐ client gives verbal consent, but unwilling or unable to sign. ☐ client gives consent to this treatment plan for psychotropic medications. Hereby give my consent to treatment with this medication.

Psychotropic Medication Consent CF 0173 C 1/15. Psychotropic Medication
I give my full consent for the use of the medication indicated above. ☐ client gives verbal consent, but unwilling or unable to sign. By signing below, i give consent for __________________________________________________________ to receive the medications listed in section a, as. ☐ client gives consent to this treatment plan for psychotropic medications. I understand that once the targeted symptom or.
![[TITLE] Understanding Psychotropic Medication A Consent Form for](https://imgv2-2-f.scribdassets.com/img/document/431008273/original/600340a19a/1707448744?v=1)
[TITLE] Understanding Psychotropic Medication A Consent Form for
I agree to notify my practitioner with any changes or problems with my medications. Hereby give my consent to treatment with this medication. I understand that i may seek additional information, and that i may. ☐ client gives consent to this treatment plan for psychotropic medications. I give my full consent for the use of the medication indicated above.
I Understand That I May Seek Additional Information, And That I May.
Hereby give my consent to treatment with this medication. I understand that once the targeted symptom or behavior is controlled, the usage of. ☐ client gives consent to this treatment plan for psychotropic medications. I agree to notify my practitioner with any changes or problems with my medications.
By Signing Below, I Give Consent For __________________________________________________________ To Receive The Medications Listed In Section A, As.
☐ client gives verbal consent, but unwilling or unable to sign. I give my full consent for the use of the medication indicated above.