Medicaid Transportation Form 2015 Pdf - Form 2015 (03/18) enrollee name: In the left column below, please check the medically necessary mode of transportation you deem appropriate for this patient: It outlines the policy procedures and. Easily customize and save as a pdf for free on. Fill and download the 2015 verification of medicaid transportation abilities form for new york. Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in.
In the left column below, please check the medically necessary mode of transportation you deem appropriate for this patient: Easily customize and save as a pdf for free on. It outlines the policy procedures and. Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in. Fill and download the 2015 verification of medicaid transportation abilities form for new york. Form 2015 (03/18) enrollee name:
Form 2015 (03/18) enrollee name: Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in. In the left column below, please check the medically necessary mode of transportation you deem appropriate for this patient: It outlines the policy procedures and. Fill and download the 2015 verification of medicaid transportation abilities form for new york. Easily customize and save as a pdf for free on.
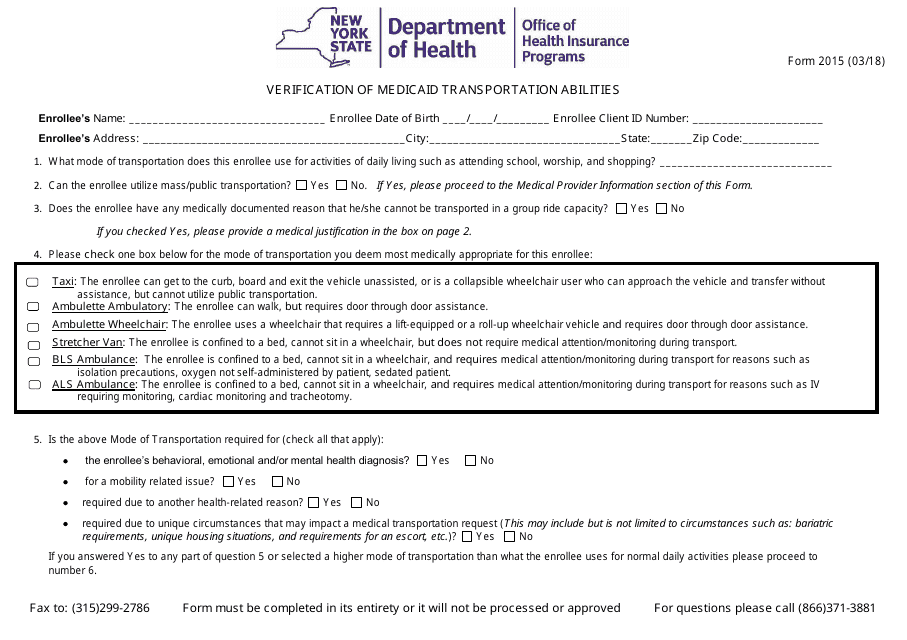
Form 2015 Fill Out, Sign Online and Download Printable PDF, New York
In the left column below, please check the medically necessary mode of transportation you deem appropriate for this patient: Easily customize and save as a pdf for free on. Fill and download the 2015 verification of medicaid transportation abilities form for new york. Form 2015 (03/18) enrollee name: It outlines the policy procedures and.
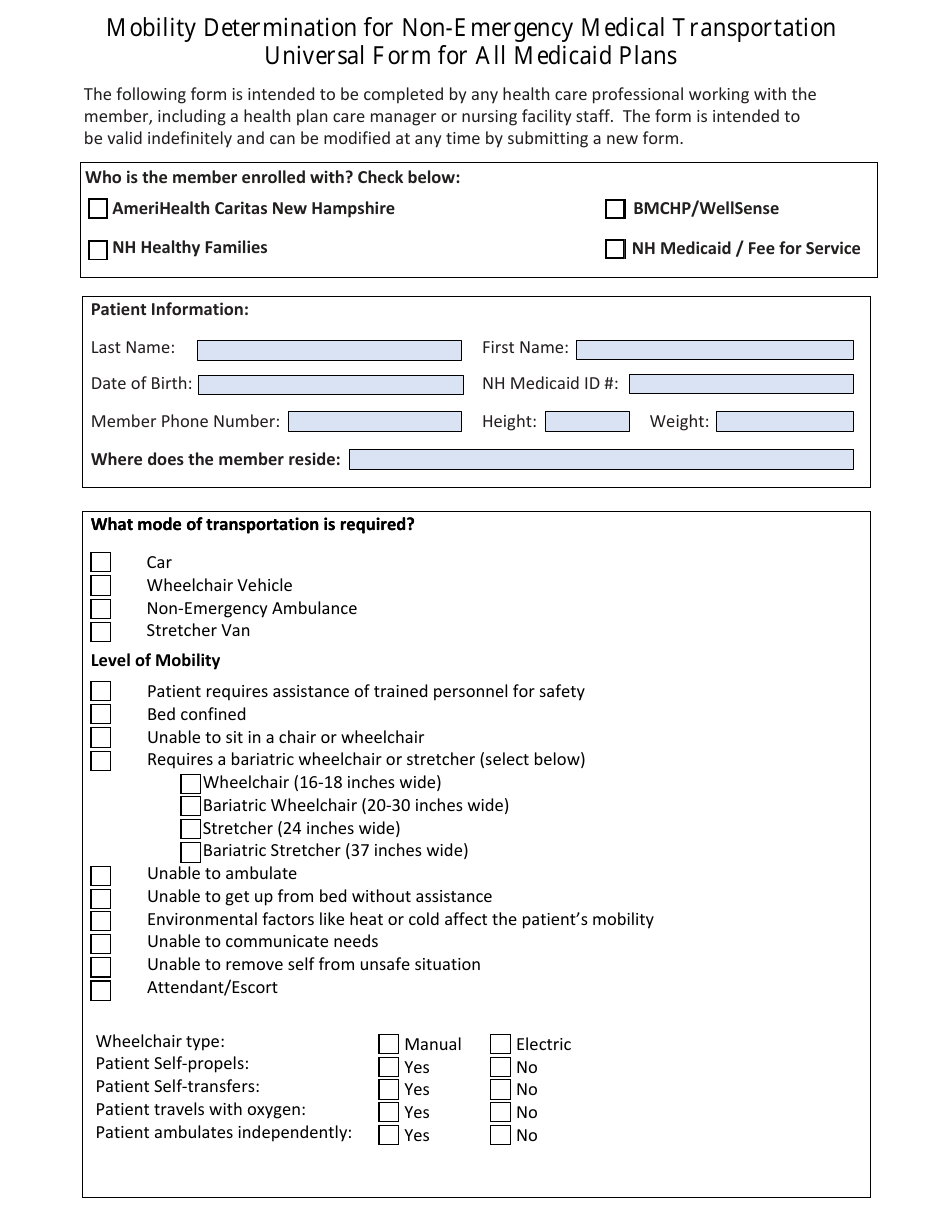
New Hampshire Mobility Determination for Nonemergency Medical
It outlines the policy procedures and. Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in. In the left column below, please check the medically necessary mode of transportation you deem appropriate for this patient: Form 2015 (03/18) enrollee name: Easily customize and save as a pdf for.
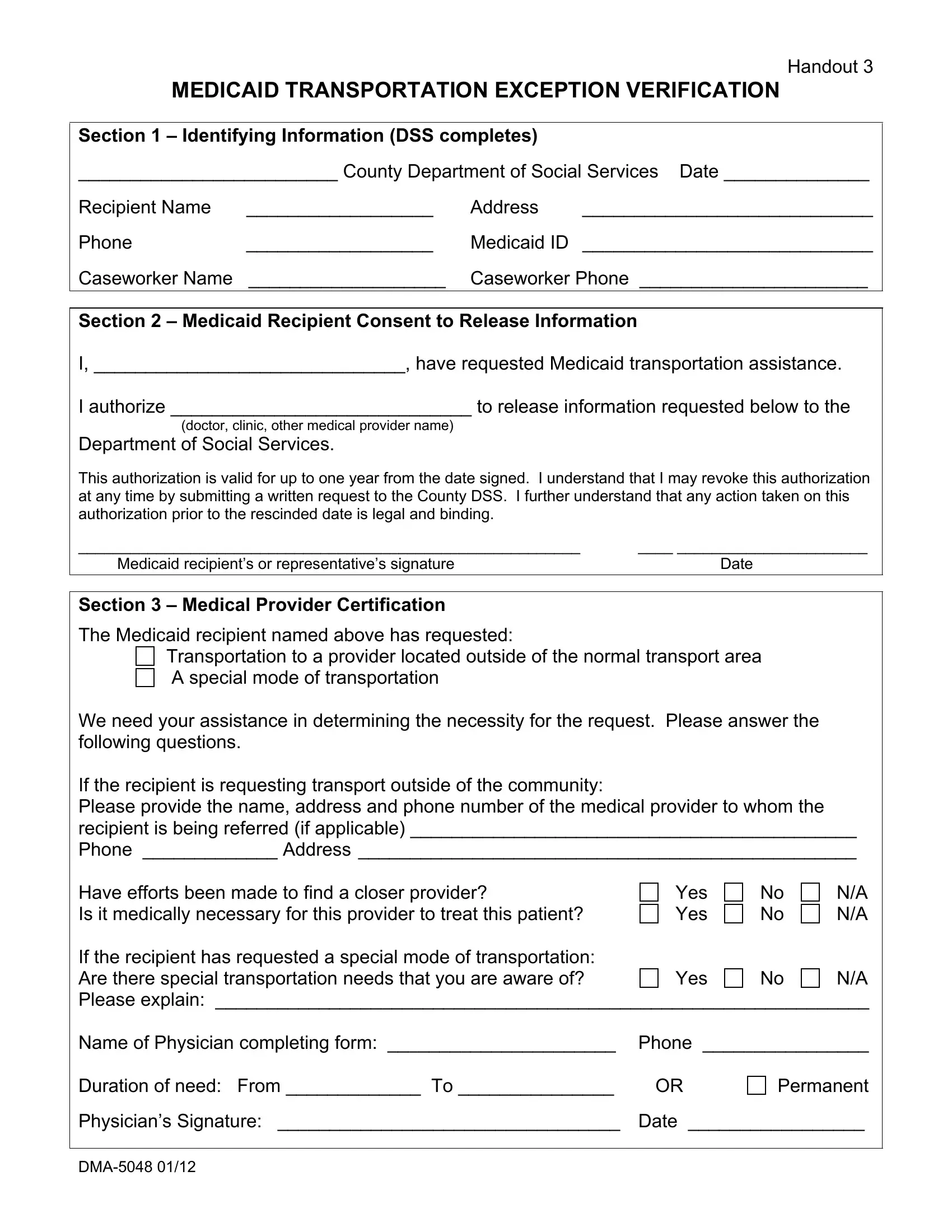
Dma 5048 Form ≡ Fill Out Printable PDF Forms Online
Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in. Fill and download the 2015 verification of medicaid transportation abilities form for new york. In the left column below, please check the medically necessary mode of transportation you deem appropriate for this patient: Easily customize and save as.
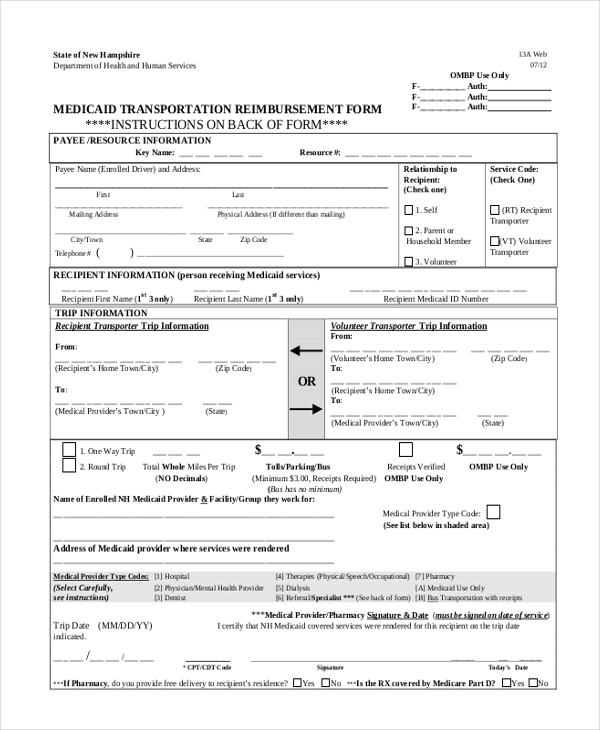
Medicaid Transportation Form Transport Informations Lane
It outlines the policy procedures and. Fill and download the 2015 verification of medicaid transportation abilities form for new york. In the left column below, please check the medically necessary mode of transportation you deem appropriate for this patient: Form 2015 (03/18) enrollee name: Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode.

Fillable Online verification of medicaid transportation abilities
Form 2015 (03/18) enrollee name: Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in. Easily customize and save as a pdf for free on. Fill and download the 2015 verification of medicaid transportation abilities form for new york. In the left column below, please check the medically.
Top Medicaid Enrollment Form Templates free to download in PDF format
Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in. Form 2015 (03/18) enrollee name: It outlines the policy procedures and. Fill and download the 2015 verification of medicaid transportation abilities form for new york. In the left column below, please check the medically necessary mode of transportation.

Medicaid transportation form 2015 online Fill out & sign online DocHub
It outlines the policy procedures and. Easily customize and save as a pdf for free on. In the left column below, please check the medically necessary mode of transportation you deem appropriate for this patient: Fill and download the 2015 verification of medicaid transportation abilities form for new york. Form 2015 (03/18) enrollee name:

Fillable Online New York State Medicaid Program Transportation Manual
Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in. It outlines the policy procedures and. In the left column below, please check the medically necessary mode of transportation you deem appropriate for this patient: Fill and download the 2015 verification of medicaid transportation abilities form for new.

Dhb 5118a Fill out & sign online DocHub
It outlines the policy procedures and. Form 2015 (03/18) enrollee name: Easily customize and save as a pdf for free on. Fill and download the 2015 verification of medicaid transportation abilities form for new york. In the left column below, please check the medically necessary mode of transportation you deem appropriate for this patient:
Form Dma5124 Medicaid Transportation Provider Documentation North
Fill and download the 2015 verification of medicaid transportation abilities form for new york. Enter all relevant medical, mental health or physical conditions and/or limitations that impact the required mode of transportation for this enrollee in. In the left column below, please check the medically necessary mode of transportation you deem appropriate for this patient: Form 2015 (03/18) enrollee name:.
Enter All Relevant Medical, Mental Health Or Physical Conditions And/Or Limitations That Impact The Required Mode Of Transportation For This Enrollee In.
In the left column below, please check the medically necessary mode of transportation you deem appropriate for this patient: It outlines the policy procedures and. Fill and download the 2015 verification of medicaid transportation abilities form for new york. Form 2015 (03/18) enrollee name: