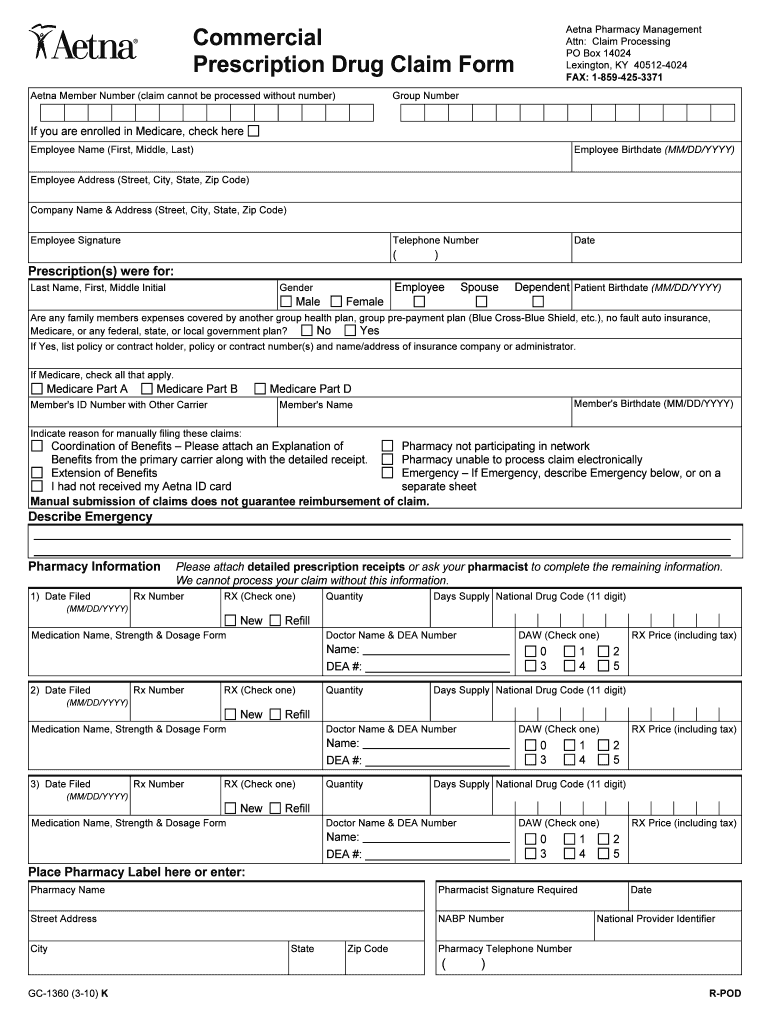
Aetna Claims Form - Refer to your plan documents to verify the coverage(s) that are available through your plan. Complete policyholder and patient information on this page. Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. All information requested in this form must be completed before your claim can be considered. Be sure to sign your claim form at the bottom of this page. For your protection california law requires notice of the following to appear on this form: Failure to complete this form. Full name of policyholder first, m.i., last. Please mail or fax completed claim form with.
Full name of policyholder first, m.i., last. Refer to your plan documents to verify the coverage(s) that are available through your plan. Please mail or fax completed claim form with. For your protection california law requires notice of the following to appear on this form: All information requested in this form must be completed before your claim can be considered. Failure to complete this form. Be sure to sign your claim form at the bottom of this page. Complete policyholder and patient information on this page. Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness.
Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Please mail or fax completed claim form with. For your protection california law requires notice of the following to appear on this form: Complete policyholder and patient information on this page. Failure to complete this form. All information requested in this form must be completed before your claim can be considered. Full name of policyholder first, m.i., last. Refer to your plan documents to verify the coverage(s) that are available through your plan. Be sure to sign your claim form at the bottom of this page.
Claim for Medical Aetna International Treatment Doc Template
Please mail or fax completed claim form with. All information requested in this form must be completed before your claim can be considered. Full name of policyholder first, m.i., last. Be sure to sign your claim form at the bottom of this page. Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service,.
Fillable Online Claim Form for Dental Treatment Reimbursements Aetna
Failure to complete this form. Please mail or fax completed claim form with. Be sure to sign your claim form at the bottom of this page. All information requested in this form must be completed before your claim can be considered. Complete policyholder and patient information on this page.
Fillable Online Claim Form for Medical Treatment Aetna
All information requested in this form must be completed before your claim can be considered. Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Be sure to sign your claim form at the bottom of this page. Please mail or fax completed claim form with. Full.
Fillable Online Claim Form for Medical Aetna International Treatment
For your protection california law requires notice of the following to appear on this form: Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Failure to complete this form. Be sure to sign your claim form at the bottom of this page. Refer to your plan.
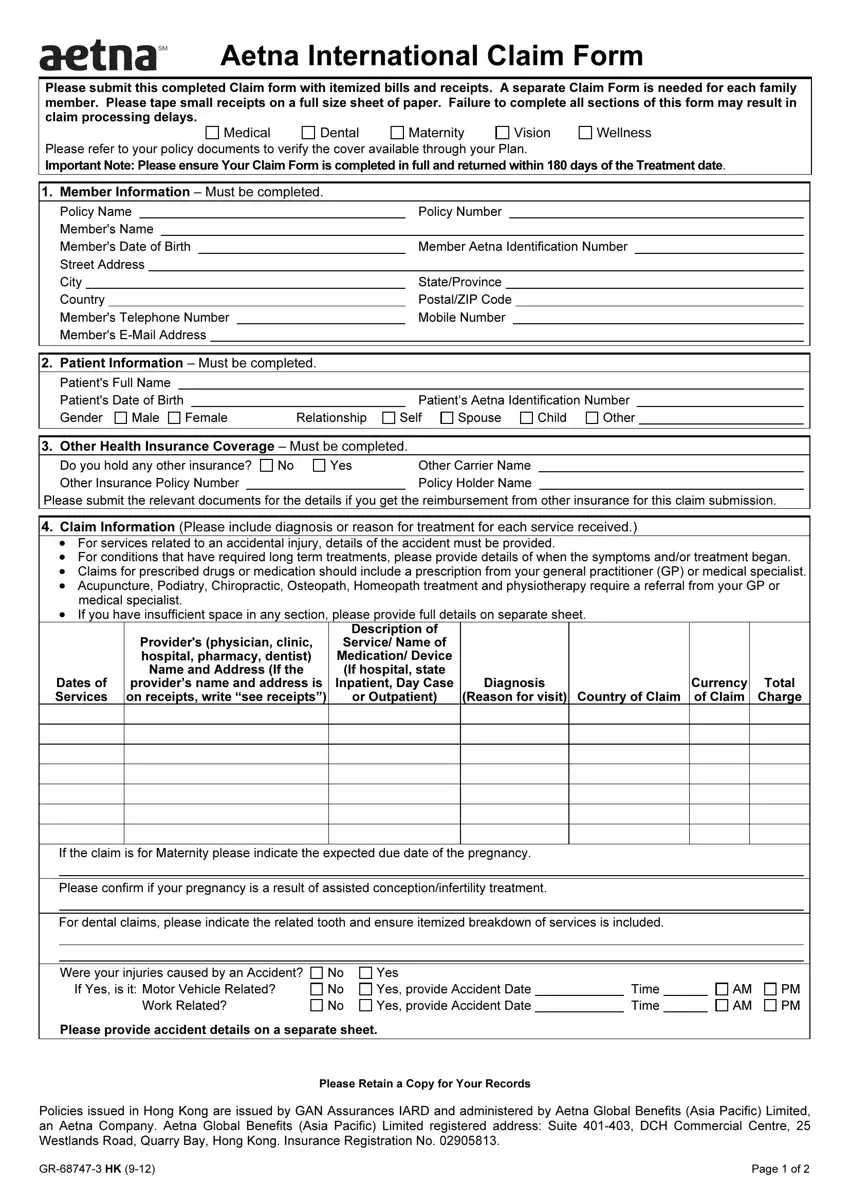
Aetna International Claim Form ≡ Fill Out Printable PDF Forms Online
All information requested in this form must be completed before your claim can be considered. Failure to complete this form. Full name of policyholder first, m.i., last. Please mail or fax completed claim form with. For your protection california law requires notice of the following to appear on this form:
Aetna claims Fill out & sign online DocHub
Full name of policyholder first, m.i., last. Refer to your plan documents to verify the coverage(s) that are available through your plan. Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. Complete policyholder and patient information on this page. All information requested in this form must.

Fillable Online Aetna Claim Form for Dental Treatment Reimbursements
Full name of policyholder first, m.i., last. Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness. All information requested in this form must be completed before your claim can be considered. Failure to complete this form. Be sure to sign your claim form at the bottom.
Aetna International Claim Form ≡ Fill Out Printable PDF Forms Online
For your protection california law requires notice of the following to appear on this form: Complete policyholder and patient information on this page. Full name of policyholder first, m.i., last. Please mail or fax completed claim form with. Be sure to sign your claim form at the bottom of this page.
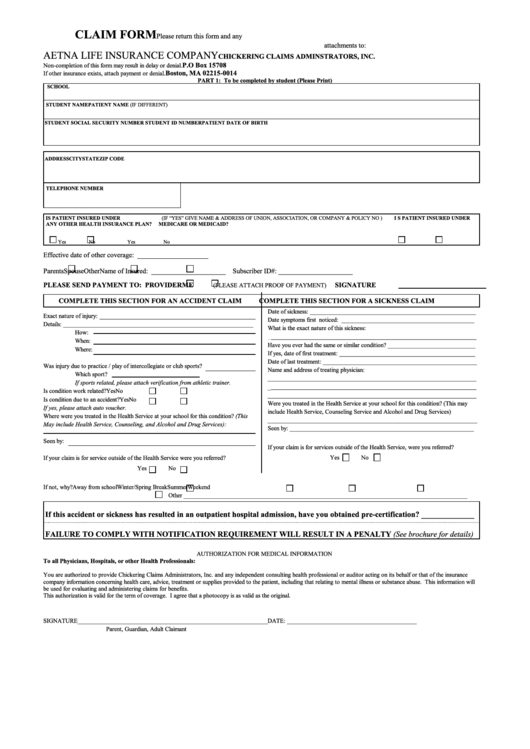
Claim Form Aetna Life Insurance Company printable pdf download
Refer to your plan documents to verify the coverage(s) that are available through your plan. Complete policyholder and patient information on this page. For your protection california law requires notice of the following to appear on this form: All information requested in this form must be completed before your claim can be considered. Be sure to sign your claim form.
Free Aetna Medical Claim Form PDF 204KB 2 Page(s) Page 2
Full name of policyholder first, m.i., last. Failure to complete this form. Refer to your plan documents to verify the coverage(s) that are available through your plan. Please mail or fax completed claim form with. All information requested in this form must be completed before your claim can be considered.
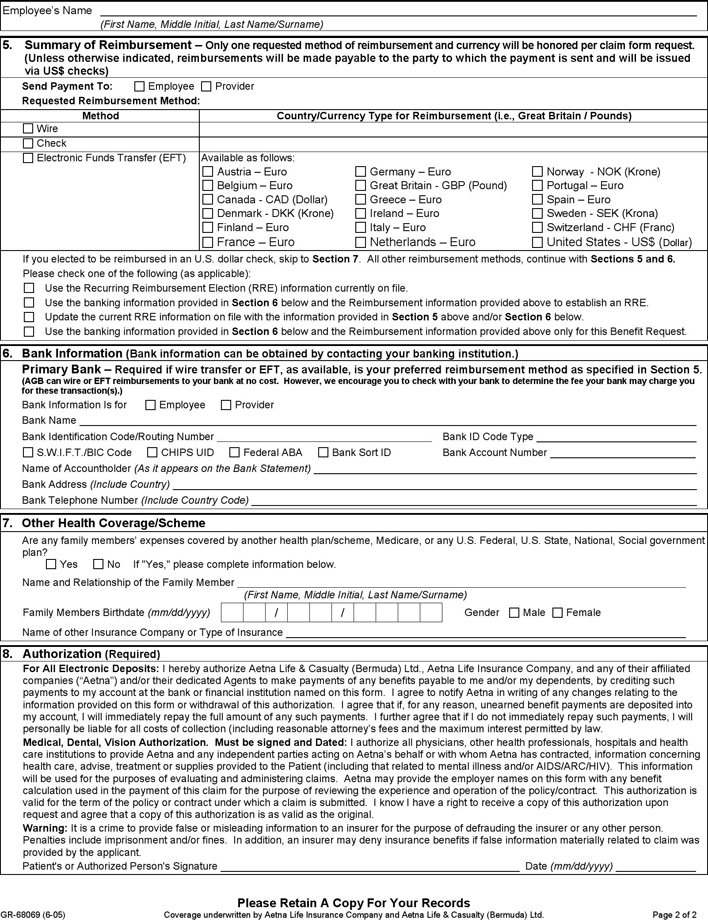
Complete Policyholder And Patient Information On This Page.
For your protection california law requires notice of the following to appear on this form: Refer to your plan documents to verify the coverage(s) that are available through your plan. Please mail or fax completed claim form with. Be sure to sign your claim form at the bottom of this page.
All Information Requested In This Form Must Be Completed Before Your Claim Can Be Considered.
Failure to complete this form. Full name of policyholder first, m.i., last. Fill out this form if you’re asking for reimbursement of a covered a medical service, dental service, eyewear, hearing aid, vaccine or fitness.